
"A Bitter Pill to Swallow”: How Healthcare Commodification Drives Inequity and the Growing Case for a Universal Healthcare System

Introduction
In February 2023, Amazon acquired OneMedical in a groundbreaking $3.9 billion deal, marking the long-anticipated entrance of the e-commerce giant into the healthcare sector. OneMedical, a popular technology-driven primary care provider, offers healthcare services to its patients through a subscription-based model. The recent acquisition not only allows Amazon to expand its healthcare offerings to its employees but also tap into the growing market for telehealth and virtual care services. The penetration of such a large and powerful corporate entity into the healthcare sector–especially primary care–is a blatant indicator of the increasing commodification of healthcare in the United States and the emphasis on market-based solutions to healthcare problems. With the acquisition consolidating Amazon's position as a major player in the healthcare market–alongside other technology giants like Google and Apple–the direction of American healthcare exists as one of our nation’s most pressing issues.
The Current State of American Healthcare
In 2020, 31.6 million Americans of all ages–roughly 10 percent of the national population–did not have health insurance. [1] Moreover, this statistic fails to account for Americans who are “underinsured”: those who have insurance but lack the necessary financial protection to cover the remaining out-of-pocket costs. The United States stands as one of the wealthiest nations in the world, yet it exists as one of the only industrialized nations without some form of universal healthcare. Furthermore, the United States spends nearly double on healthcare expenditures than comparable countries, yet has marginally worse health outcomes. [2]
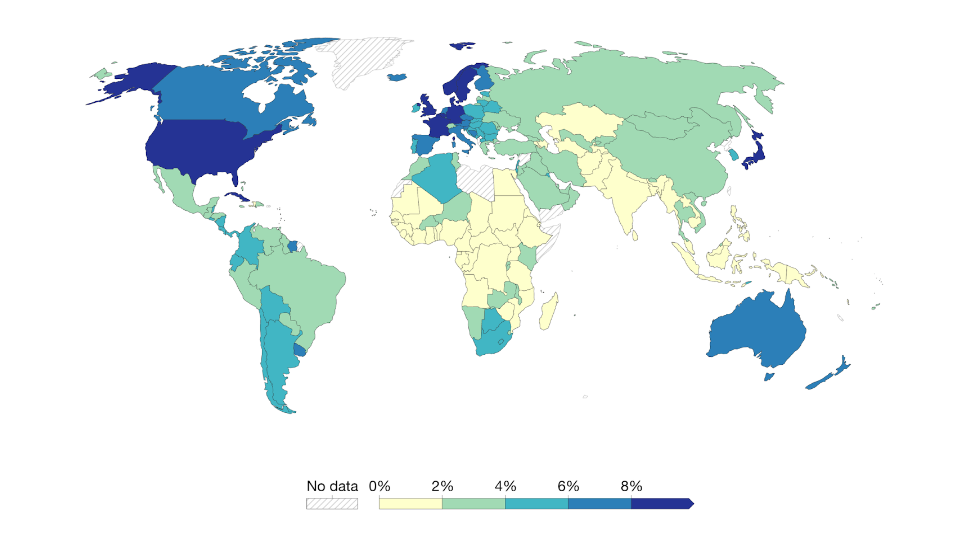
Figure 1 Total healthcare expenditure as the share of GDP [3]
As healthcare premiums continue to soar while return on investment seems to diminish, the discussion of reforming our healthcare system is of much contention. Despite the significant spread of healthcare coverage under President Obama’s Affordable Care Act (ACA), our system is far from perfect. The implementation of a universal healthcare system in the United States would provide coverage to a sizeable, unhealthy portion of society and yield a multitude of economic and social benefits. The system would eliminate discrimination based on income and pre-existing conditions and reduce crime by providing widespread access to care. Furthermore, increased economic productivity and cost reduction refute the financial concerns of those who argue for contrary systems.
The Social Case for a Universal Healthcare System
The universal healthcare system revolves around solidarity. Historically, for-profit insurance companies price out low-income families, leaving them unable to pay out the high costs demanded of them. According to surveys and meta-analyses conducted by the Kaiser Family Foundation (KFF), families with low incomes and people of color are more likely to be uninsured. [4] The American healthcare system only furthers inequality by prioritizing corporate interest over the well-being of the American citizen. This phenomenon is described as “health disparity,” defined by The Centers for Disease Control and Prevention (CDC) as “preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations.” [5] A universal healthcare system will eliminate these disparities as everyone will be ensured access to healthcare no matter their financial background or identity.
The traditionally conservative solution to our healthcare crisis advocates against universal healthcare and even promotes repealing the established ACA. This solution will only further inequality and health disparities by putting people with pre-existing conditions in a more vulnerable place. Before the introduction of the ACA, insurance companies “could deny coverage, charge higher premiums, and/or limit benefits to individuals based on pre-existing conditions.” [6] Privatized, for-profit insurance companies were denying 1 in 2 Americans with pre-existing conditions insurance or coverage for illnesses caused by these conditions. [7] This profit-driven over care-driven model of insurance left Americans without healthcare when they needed it most. However, beginning in 2014, the ACA granted protection to individuals with pre-existing conditions as it prohibited insurers from using health status to determine healthcare eligibility. [8] A universal healthcare system would make certain that our society would continue valuing profit over its citizens’ health.
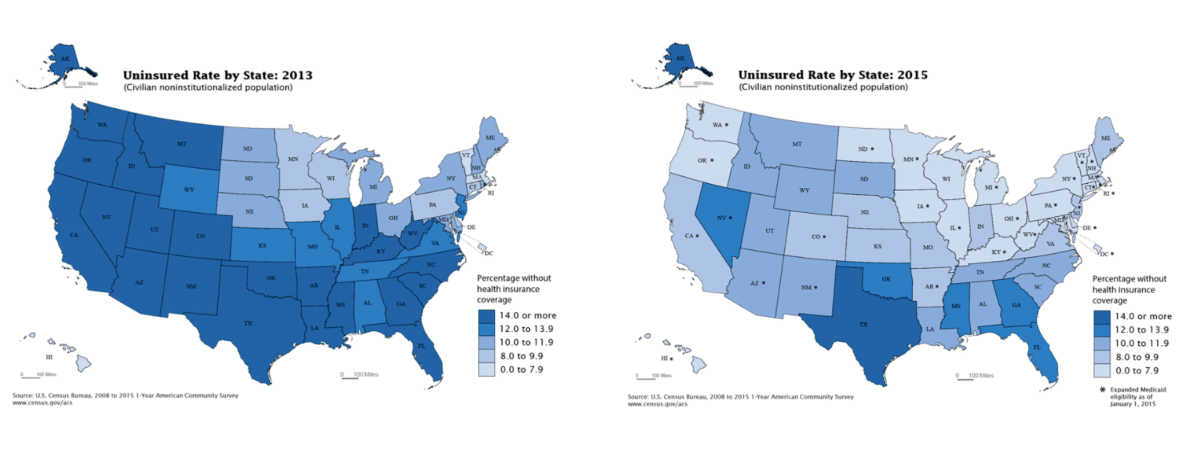
Figure 2 Healthcare Coverage Pre and Post ACA [9]
Lastly, the majority of individuals who are currently or have previously been incarcerated have severe unattended medical issues. 3 out of 5 state prisoners and jail inmates have some sort of substance abuse problem; half of all state and federal prisoners are experiencing severe emotional or psychological turmoil, or have a prior record of mental health issues. [10] Although American jail and prison services provide treatment for inmates with health conditions, a much safer and cost-effective solution would be to provide coverage for treatment before crimes are committed, emphasizing preventative care over intervention. When analyzing the relationship between substance abuse treatment facilities and crime, researchers found that there is a statistically significant positive correlation between the reduction of drug abuse and the reduction of violent behavior as well as property crimes committed to fund addiction.[11] Providing every American citizen healthcare, subsequently allowing every American to receive medical treatment, will have tremendous social benefits for our society, reducing crime while increasing safety.
The Economic Case for a Universal Healthcare System
Furthermore, a strong economic case exists for implementing a universal healthcare system. The foremost evidence is that healthcare spending would be reduced by a drastic amount. Simulations of progressive financing under an improved version of the Medicare for All Act assert the following: “Under the single-payer system created by HR 676, the U.S. could save an estimated $592 billion annually by slashing the administrative waste associated with the private insurance industry ($476 billion) and reducing pharmaceutical prices to European levels ($116 billion).” [12] Under the same study, the progressive redistribution of obsolete tax funding sources and government spending garnered hundreds of billions of dollars readily available for healthcare expenditures. Moreover, of the 37 nations part of the OECD (Organization for Economic Co-operation and Development), the United States is the only nation that does not have universal health care either in practice or by constitutional right. [13] Nations part of the OECD spend fractions of what the United States pays for healthcare. Two countries that provide a form of universal health coverage, Canada and the United Kingdom, spent 47% and 42% of what the United States did per capita in 2017, respectively. South Korea, another nation with universal coverage, spent only 28%. [14]
Moreover, not only will government spending be significantly lowered, but also healthcare costs will decrease at the consumer level. Done right, universal healthcare would lower costs while letting the government leverage healthcare dollars to respond to public health, invest in disease prevention, and modernize primary care delivery without the assistance of powerful corporate institutions. [15] Additionally, the United States economy loses between $65 billion and $130 billion annually due to poor health and premature deaths among the uninsured, leading to worker absence and economic loss. This issue could be resolved by ensuring access to preventative healthcare treatment for everyone. [16] The primary objections to universal healthcare are rooted in economic concerns, particularly the fear of increased taxes. However, experts argue that investing in universal healthcare is worthwhile and would bring significant returns, as demonstrated by the evidence presented earlier. By promoting the welfare of all Americans and redistributing expenditures to more important areas, the country would see a greater return on investment than what would be lost through taxes. [17]
Additionally, a large concern cited by antagonists of a universal healthcare system is that the quality of care would be diminished, lowering the value of healthcare. This point is most commonly backed by the speculation of increased wait times for medical treatment brought on by universal healthcare. Despite the opposite being true, the United States, in its current privatized healthcare system, actually ranks far lower in The Healthcare Access and Quality (HAQ) Index–which is calculated by differences in preventing amenable mortality–than all Nordic countries that have implemented universal healthcare. [18] Citing wait times is an extremely ineffective measure of the quality of healthcare compared to the HAQ index. In fact, the inefficiency of the United States healthcare system was on full display during the COVID-19 pandemic. In 2020 alone, 212,000 deaths could have been prevented, and $105.6 billion of medical expenses associated with COVID-19 hospitalization could have been averted by a Medicare for All system. [19]
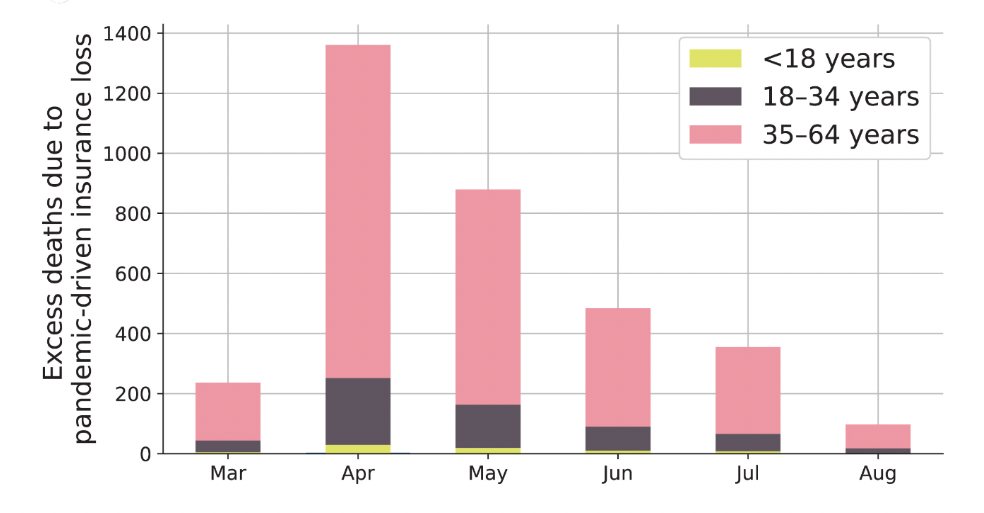
Figure 3 Preventable Deaths During Covid-19 Pandemic Due to Lack of Healthcare Insurance [20]
An Overview
So many countries have set a remarkable precedent in implementing a universal healthcare system that ensures each of its citizens has a right to quality healthcare. It is astounding that the United States, which prides itself in providing its citizens the greatest chances at upward mobility, has failed to follow suit. Outdated ideologies that reject the reformation of the capitalist policies that drive American economics have harmed so many attempts at progress within our institutions. Our failures in healthcare stand as a prime example of this stagnancy. Our current healthcare system provides excellent commentary on how our free market and corporate institutions have jeopardized American health and equality for their own economic benefit. The case for a universal healthcare system continues to grow stronger as national disparities grow larger. Too long have Americans stayed idle in allowing institutions to perpetuate systemic inequity. The time for change is long overdue.
Cha, Amy E., and Robin A. Cohen. “National Health Statistics Reports.” Demographic Variation in Health Insurance Coverage: United States, 2020, National Health Statistics Reports, vol. 169, 11 Feb. 2022, https://www.cdc.gov/nchs/data/nhsr/nhsr169.pdf ↩︎
Kurani, Nisha, and Cynthia Cox. “What Drives Health Spending in the U.S. Compared to Other Countries.” Peterson-KFF Health System Tracker, Peterson-KFF, 20 July 2021, https://www.healthsystemtracker.org/brief/what-drives-health-spending-in-the-u-s-compared-to-other-countries/ ↩︎
Ortiz-Ospina, Esteban and Max Roser. "Healthcare Spending.” OurWorldInData.org, 2017, 'https://ourworldindata.org/financing-healthcare ↩︎
Tolbert, Jennifer, et al. “Key Facts about the Uninsured Population.” KFF, 12 Nov. 2020, https://www.kff.org/uninsured/issue-brief/key-facts-about-the-uninsured-population/ ↩︎
Artiga, Samantha, and Nambi Ndugga. “Disparities in Health and Health Care: 5 Key Questions and Answers.” KFF, 12 May 2021, https://www.kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/#:~:text=Healthy People 2020 defines a,health based on their racial ↩︎
“At Risk: Pre-Existing Conditions Could Affect 1 in 2 Americans.” ASPE, Office of the Assistant Secretary for Planning and Evaluation, 31 Oct. 2011, https://aspe.hhs.gov/reports/risk-pre-existing-conditions-could-affect-1-2-americans-0 ↩︎
“At Risk: Pre-Existing Conditions Could Affect 1 in 2 Americans.” ASPE, Office of the Assistant Secretary for Planning and Evaluation, 31 Oct. 2011, https://aspe.hhs.gov/reports/risk-pre-existing-conditions-could-affect-1-2-americans-0 ↩︎
“At Risk: Pre-Existing Conditions Could Affect 1 in 2 Americans.” ASPE, Office of the Assistant Secretary for Planning and Evaluation, 31 Oct. 2011, https://aspe.hhs.gov/reports/risk-pre-existing-conditions-could-affect-1-2-americans-0 ↩︎
U.S. Census Bureau, 2008 to 2015, 1-Year American Community Survey ↩︎
Doleac, Jennifer L. “New Evidence That Access to Health Care Reduces Crime.” Brookings, Brookings, 3 Jan. 2018, https://www.brookings.edu/blog/up-front/2018/01/03/new-evidence-that-access-to-health-care-reduces-crime/ ↩︎
Doleac, Jennifer L. “New Evidence That Access to Health Care Reduces Crime.” Brookings, Brookings, 3 Jan. 2018, https://www.brookings.edu/blog/up-front/2018/01/03/new-evidence-that-access-to-health-care-reduces-crime/ ↩︎
Friedman, Gerald. Funding HR 676: The Expanded and Improved Medicare for All Act How we can afford a national single-payer health plan. Pnhp.org. The University of Massachusetts, 31 July 2013, http://www.pnhp.org/sites/default/files/Funding HR 676_Friedman_7.31.13_proofed.pdf ↩︎
“Universal Healthcare Pros and Cons - Is It a Human Right?” Right to Health Care, ProCon.org, 17 Feb. 2022, https://healthcare.procon.org/ ↩︎
“Universal Healthcare Pros and Cons - Is It a Human Right?” Right to Health Care, ProCon.org, 17 Feb. 2022, https://healthcare.procon.org/ ↩︎
Berwick, Donald M. “Stop Fearmongering about 'Medicare for All.' Most Families Would Pay Less for Better Care.” USA Today, Gannett Satellite Information Network, 22 Oct. 2019, https://www.usatoday.com/story/opinion/2019/10/22/medicare-all-simplicity-savings-better-health-care-column/4055597002/ ↩︎
“Universal Healthcare Pros and Cons - Is It a Human Right?” Right to Health Care, ProCon.org, 17 Feb. 2022, https://healthcare.procon.org/ ↩︎
Friedman, Gerald. Funding HR 676: The Expanded and Improved Medicare for All Act How we can afford a national single-payer health plan. Pnhp.org. The University of Massachusetts, 31 July 2013, http://www.pnhp.org/sites/default/files/Funding HR 676_Friedman_7.31.13_proofed.pdf ↩︎
Kurani, Nisha, and Emma Wager. “How Does the Quality of the U.S. Health System Compare to Other Countries?” Health System Tracker, Peterson-KFF, 24 Feb. 2022, https://www.healthsystemtracker.org/chart-collection/quality-u-s-healthcare-system-compare-countries/ ↩︎
Galvani, Alison P, et al. “Universal Healthcare as Pandemic Preparedness: The Lives and ... - PNAS.” PNAS.org, Proceedings of the National Academy of Sciences of the United States of America, 13 June 2022, https://www.pnas.org/doi/10.1073/pnas.2200536119 ↩︎
Galvani, Alison P, et al. “Universal Healthcare as Pandemic Preparedness: The Lives and ... - PNAS.” PNAS.org, Proceedings of the National Academy of Sciences of the United States of America, 13 June 2022, https://www.pnas.org/doi/10.1073/pnas.2200536119 ↩︎

