
Examining the U.S. Response to Covid 19: An Externalities-Based Approach
By Jay Patel, From Northeastern University
COVID-19 is an infectious disease caused by the SARS-CoV-2 virus. Between 2020 and 2023, Covid-19 was declared a global pandemic. To reduce the transmission of the disease, initially, countries imposed regulations that severely restricted economic activity, plunging global markets into a deep recession. In the United States alone, COVID-19 is estimated to have caused up to $14 Trillion in losses (Hlávka, 2023).1 Despite these efforts, as of October 6th, 2023, the death toll of Covid-19 is approaching 7,000,000 people (WHO, 2023).2 Throughout the pandemic, individual actions could hold both positive and negative societal implications. In economics, this is referred to as an ‘externality,’ or a cost or benefit to an uninvolved third party, arising as an effect of another party's activity. This article analyzes the United States' response to the pandemic, emphasizing the public policy initiatives launched to confront externalities linked to COVID-19. By drawing comparisons with peer high-income nations, this article aims to assess the effectiveness of these policies and identify distinctive characteristics of the United States' approach.
Positive Externalities and Vaccine Subsidization:
Positive Externalities occur when a certain private actor’s individual actions provide some type of benefit to society. The private actor, however, will not be compensated for these benefits to society, and as such the private actor may reduce the amount of the beneficial activity they engage in. We can see the concept of positive externalities throughout various facets of society. For instance, commuters who use public transportation, as opposed to driving, generate a positive externality by reducing the traffic for other commuters. These Public Transportation users, however, are not compensated for their efforts to reduce traffic. As such, there is often a less than ideal number of people who utilize public transportation.
During the first year of the COVID-19 pandemic, the development of a vaccine was a primary goal of the US Federal Government’s policy response. Traditionally, economic theory describes the private research and development of vaccines as creating a positive externality, as the societal benefits of creating such vaccines lay beyond the private profits realized by pharmaceutical firms from the sale of vaccines, leading to an under-supply of vaccines. As described by health economists Jagannath M. Muzumdar and Richard R. Cline, the research and development of vaccines have two primary externalities:
(1) vaccination helps protect even those individuals not receiving the vaccine by reducing the transmission of a given disease and (2) reductions in the burden of infectious disease in the 20th century have been linked to considerable economic expansion during that period.
(Muzumdar & Cline, 2009, pg. 06) 3
The development of COVID-19 vaccines were expected to produce similar externalities, namely by reducing the transmission of the virus, which was anticipated to bring an end to mitigation measures that had been restricting the American and global economies.
Ultimately, as is the case with positive externalities, private pharmaceutical firms are not themselves compensated for generating such social benefits in excess of their private profits, leading to the underproduction of vaccines, compared to the socially efficient level. To counter this, governments typically subside to the production of vaccines, as was done during the Covid-19. Researchers found that between March 2020 and March 2022, the Federal government invested $2.365 Billion in COVID-19 mRNA research and development (Lalanit Et al., 2023, pg. 04).4
Demand-Side Vaccine Public Provision:
In addition to supply-side subsidies to increase vaccine production, the Federal Government also provided demand-side subsidies to encourage vaccine consumption or inoculation. Inoculation also develops a positive externality by creating a social benefit beyond the private gain one receives through vaccination. As described by researchers in the Frontiers in Public Health journal:
By choosing to be vaccinated, an individual protects themself but also protects their community by preventing disease transmission.
(Wagner Et al., 2020, pg.01) 5
To encourage inoculation amongst the population and capture the positive externality of vaccination, the federal government, in a highly unusual move considering the market-based system underlying US Healthcare, announced that the vaccine would be provided free of charge to all citizens as a public provision (Gumbrecht & Thomas, 2020).6 Between 2020 and 2022, to fund this public provision of vaccines, researchers found that the Federal Government purchased $29.209 Billion of COVID-19 mRNA vaccines (Lalanit Et al., 2023, pg. 04).4
See below for full cost breakdown of vaccine R&D and provision by the U.S Federal Government (Lalanit Et al., 2023, pg. 04): 4
Results of Vaccine Subsidies:
In total, the US Federal Government expensed $31.912 Billion in vaccine subsidies, including both supply-side support for vaccine research and development and demand-side public provision to increase inoculation. Research generally suggests that the subsidization of vaccines in the US was effective in reducing the transmission, hospitalization, and death caused by Covid-19. In Particular, between December 12, 2020, and November 30, 2021, the US vaccination program was successful in averting 35,903,646 Infections, 10,319,961 Hospitalizations, and 1,087,191 Deaths (Schneider, Et al., 2021).7 In the below time-series between October 2020 and December 2021, the gap between the observed number of deaths, given the administration of the Covid vaccine, and the projected number of deaths without the administration of the Covid vaccine is particularly striking (Schneider, Et al., 2021).7
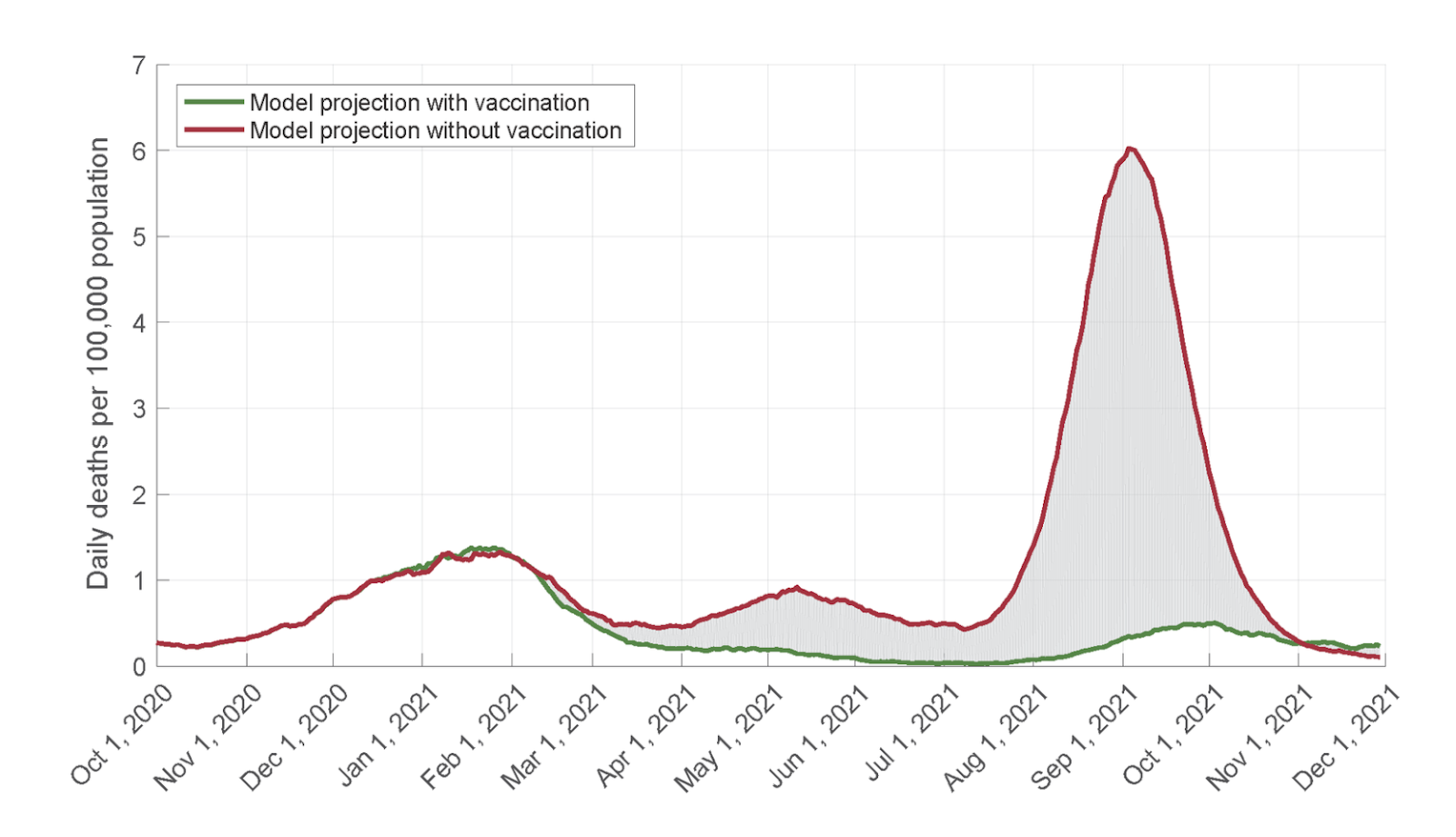
For instance, in September 2021, the projected number of COVID-19 deaths without vaccination was 24 times higher than the projected number of deaths with vaccination. Simply put, the subsidization of vaccine development and deployment was critical to reducing Covid-19 deaths.
Comparative Analysis and Excess Mortality:
While these absolute figures might appear to solidify the effectiveness of the United State’s vaccine response, to ascertain a true understanding of the program’s efficacy we must compare the US vaccine program with that of its peer nations. When one observes the below time series, developed using data from OurWorldinData.org, one can see that the United States experienced a higher excess mortality rate than 14 of its peer high-income nations, especially following the authorization of the first COVID-19 vaccines in December 2020 (Mathieu, E., Et al., 2023).8
The excess mortality rate describes, relative to COVID-19, the excess deaths attributable to COVID-19, compared to the level of death that would have been witnessed without COVID-19. Thus, a country with a higher excess mortality rate can attribute a larger number of its populous deaths to COVID-19.
Ultimately, while it is true that the United States’s subsidization of vaccination production and inoculation created a large absolute benefit in saving lives, the number of lives saved in the United States, compared to other peer nations, adjusting for population size differences, was poor. Additionally, when one examines the below time series, also developed using data from OurWorldinData.org, one can see that, out of the same group of 14 peer high-income nations, the United States achieved the lowest rate of full vaccination (Mathieu, E., Et al., 2023).8
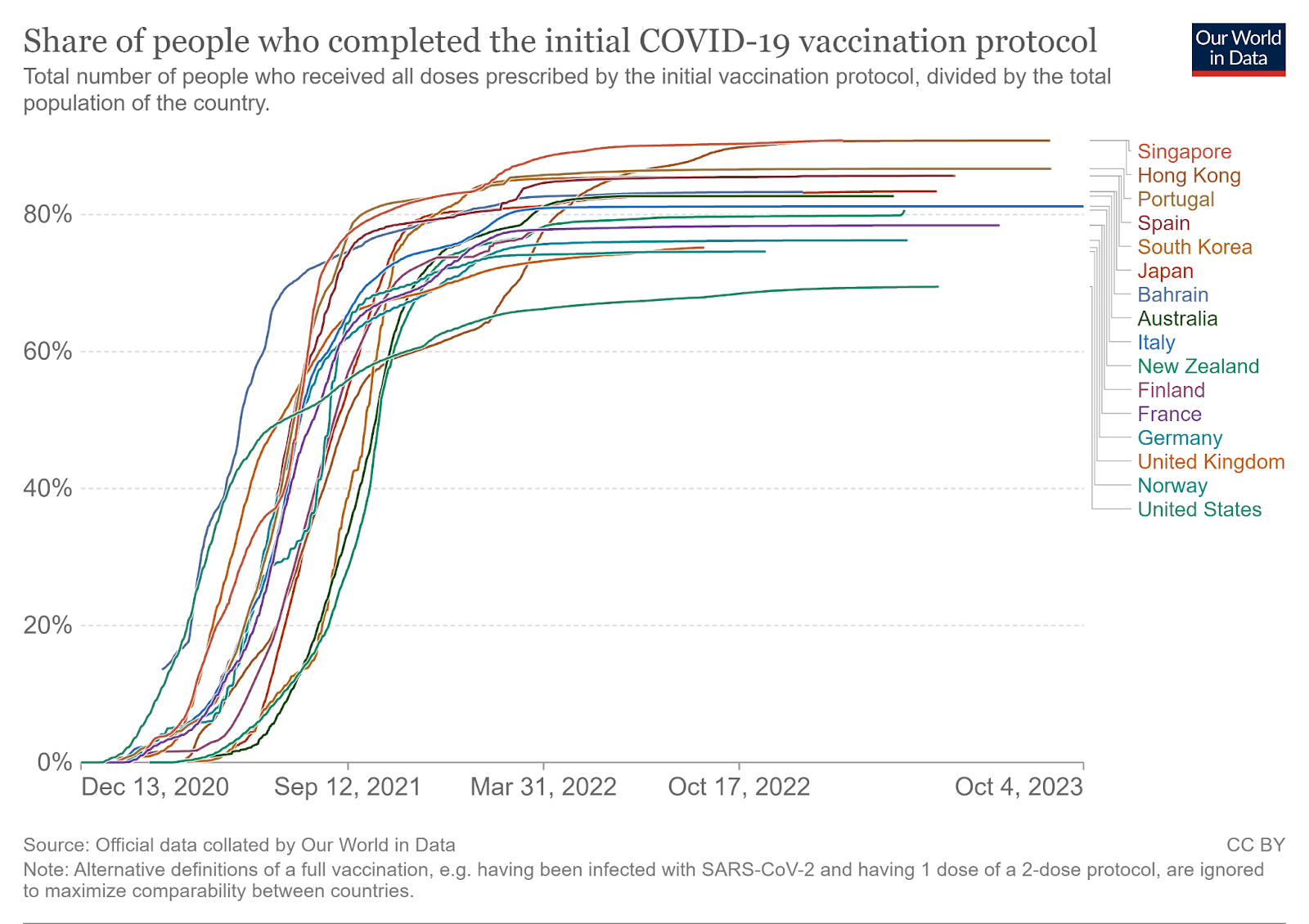
Simply stated, with less of its population vaccinated against Covid-19, it is logical that death rates from Covid-19 would be higher in the United States, compared to that of its peer high-income nations, leading to higher rates of excess mortality. For additional evidence linking the relationship between excess mortality and vaccination rates, researchers found that in the U.S. states with the highest vaccination rates, excess mortality was actually comparable to or even less than those of the United State’s peer nations. One study found that the 10 U.S. states with the highest rates of vaccination had less excess mortality than several countries who had less excess mortality than the United States as a whole. This included countries like Denmark, Germany, the Netherlands, Austria, Italy, and Finland-
“US excess all-cause mortality exceeded Covid-19 mortality at 145/100 000 and exceeded peer countries in all periods, as did excess all-cause mortality in the least-vaccinated states. However, the 10 most-vaccinated states had excess all-cause mortality comparable with or less than that of several peer countries over Delta and Omicron combined (eg, Denmark, Germany, the Netherlands, Austria, Italy, Finland).”
(Bilinski A., Et al., 2022, Pg. 1) 9
Misinformation and Negative Externalities:
Now, logically, one must also ask why exactly the United States experienced a lower rate of full vaccination, compared to that of its peer high-income nations. As is shown below, researchers have found that US media sources produce the world's second-highest level of COVID-19 misinformation (Al-Zaman S., Et al., 2021, pg. 11).10
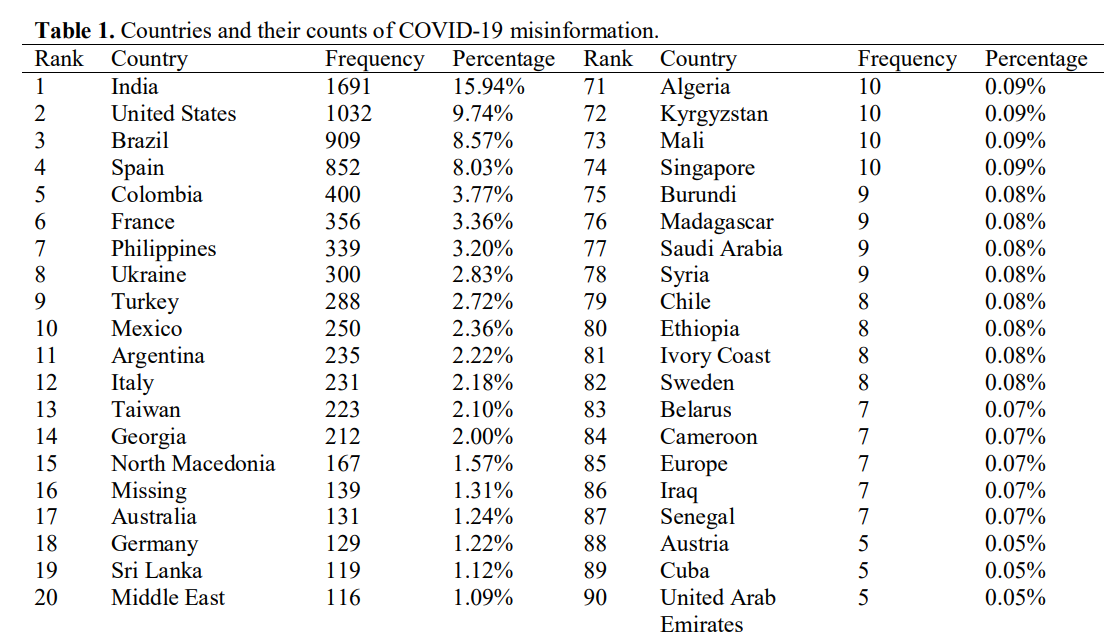
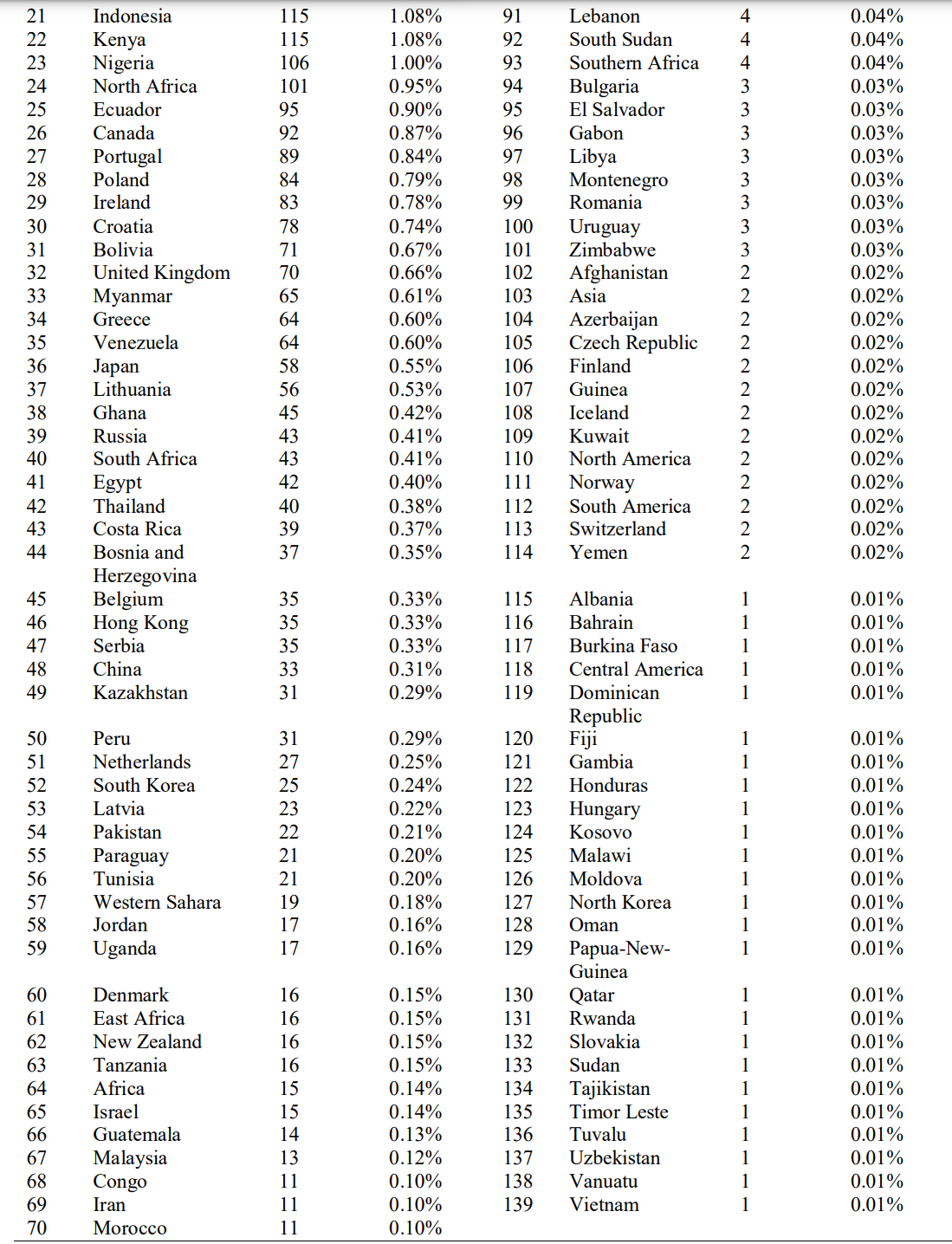
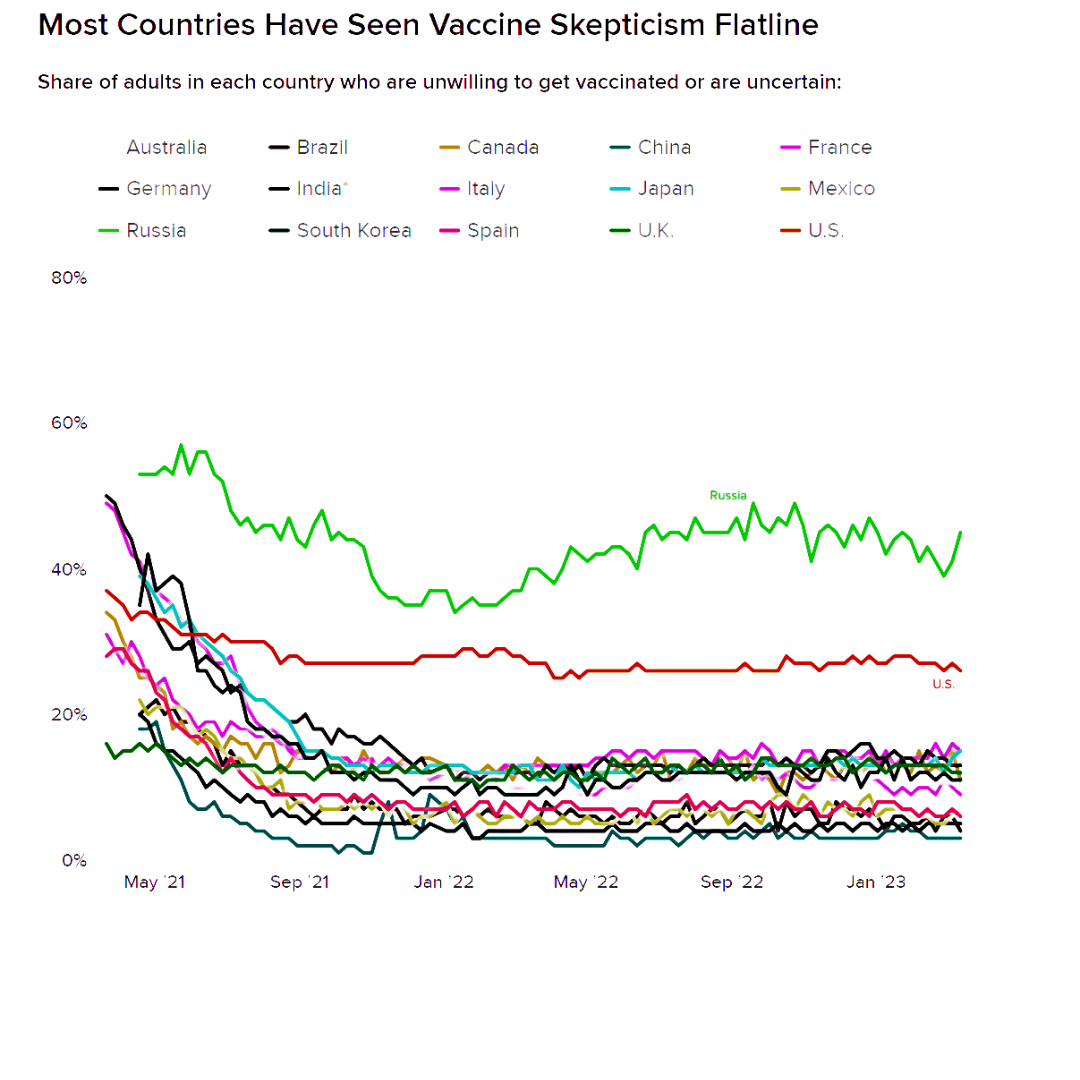
Misinformation produces negative externalities- that is, there is a cost to society as misinformation is propagated, but the propagators of misinformation do not bear such costs themselves. In particular, Covid-19 misinformation is often centered around incorrect and misleading information about Covid-19 vaccines. This creates a social cost by increasing vaccine hesitancy in the populace exposed to the misinformation. Given the strong prevalence of COVID-19 misinformation in the United States, one would expect the weight of the negative externality of vaccine hesitancy to be larger in the United States, compared to her peer nations. As displayed below, the percentage of the population unwilling to get vaccinated is significantly greater than that of other high-income nations (Coleman J., 2023).11
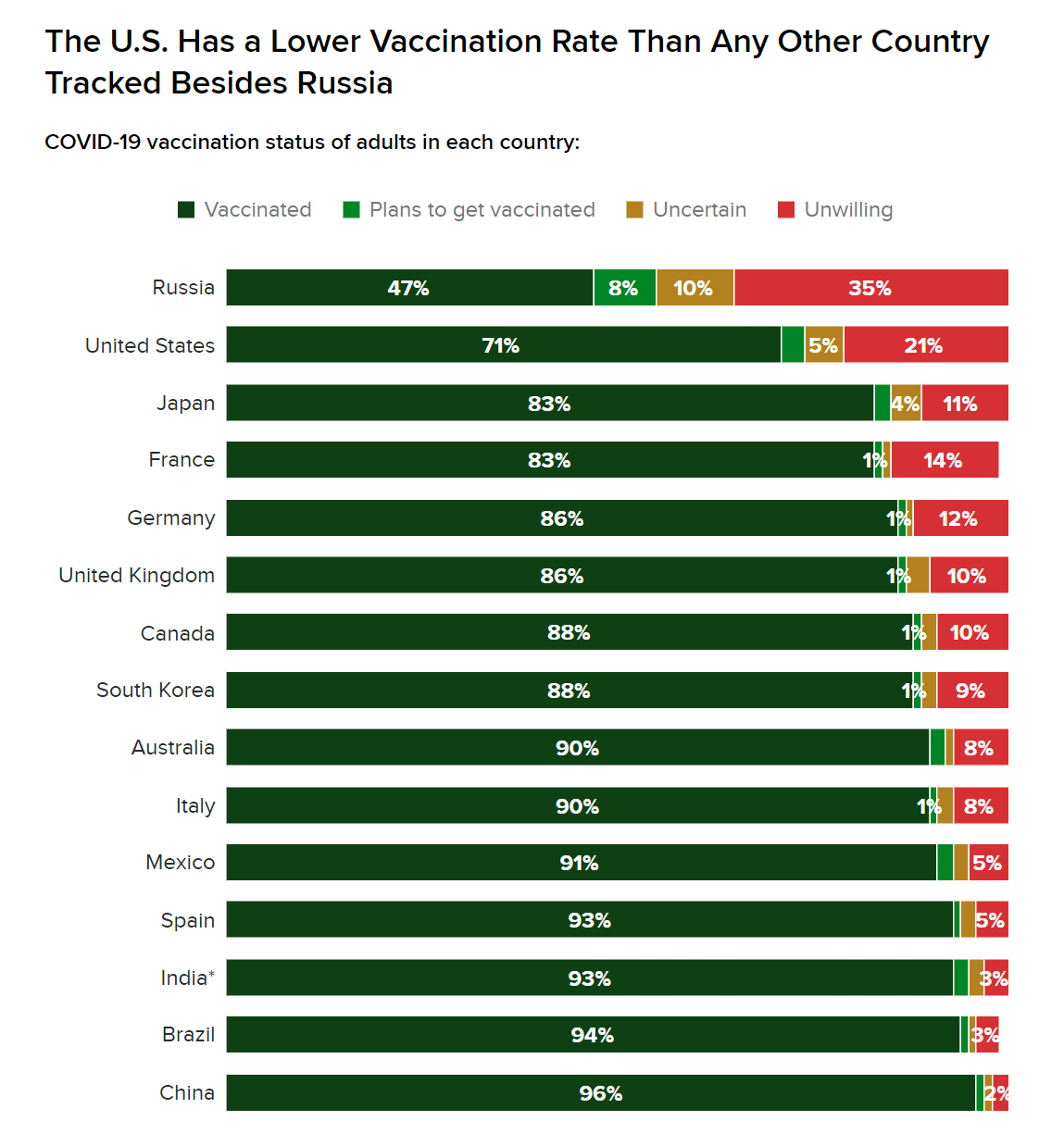
Additionally, as seen in Exhibit G, behind Russia, the US is the most vaccine-skeptical high-income nation by a significant margin (Coleman J., 2023).11
Role of National Values in Developing a Policy Response
Given that misinformation has created such a significant negative externality in the United States through rising rates of vaccine hesitancy and skepticism, from a neoclassical economic perspective, the US government should take public policy measures to reduce the production and/or consumption of misinformation. Reducing vaccine misinformation would further reduce the cost vaccine hesitancy places on society, relative to prolonging the Covid-19 pandemic, increasing pandemic death rates, etc.
Other high-income nations have opted to take this heavy-handed regulatory approach. For instance, in April of 2023, the Digital Services Act, passed by the European Parliament, came into effect across the EU. The regulation requires media firms with at least 45 million monthly users to put into place internal systems that monitor and remove misinformation and propaganda (Freedman R., 2023).12 In the US, however, the concept of regulating misinformation sparks incredible contention. As described by the Congressional Research Service,
“The Supreme Court has recognized that false statements may not add much value to the marketplace of ideas. Even so, there is a concern that by prohibiting false speech, the government would… cause people to self-censor out of fear of violating the law…The Court has suggested the government may not regulate false ideas, and even false factual statements receive some constitutional protection.
(Brannon V.C., 2022) 13
Thus, while other high-income nations have chosen to regulate misinformation to reduce the social cost of vaccine hesitancy, the United States has chosen to value freedom of speech and personal liberty, thereby sacrificing social efficiency. Ultimately, this difference in COVID response, relative to the regulation of misinformation, between the United States and other High-Income Nations is due to a difference in national values. European nations within the EU are more socially inclined than the United States and are thereby willing to give up personal liberty and freedom to achieve greater social efficiency. The United States, being more individualistic, values such as personal liberty and freedom over social efficiency, leading to a difference in national response.
The United States' response to the COVID-19 pandemic was marked by commendable efforts to capture the positive externalities associated with vaccine development and inoculation. Substantial investments in vaccine research and development, coupled with the provision of vaccines free of charge, demonstrated a commitment to public health and economic recovery. However, this success was tempered by the negative externalities arising from rampant misinformation. The failure to regulate misinformation, despite its adverse effects on vaccination rates, reflects a fundamental difference in national values between the United States and its peer countries. While other high-income nations have opted for regulatory approaches to prevent the spread of misinformation, the United States has prioritized individual liberty and freedom of speech, even at the cost of public health. This stark contrast in pandemic response strategies underscores the influence of national values and ideology on public policy, even during critical periods of national emergency. In summary, the United States' response to the COVID-19 pandemic exhibited a dual character: remarkable achievements through vaccine development and provision, counterbalanced by the adverse impact of misinformation. The trade-off between personal liberty and social efficiency became emblematic of the nation's individualistic values, shaping its response to this global health crisis.
Sources:
- Hlávka, J., & Rose, A. (2023, May 25). Covid-19’s total cost to the U.S. economy will reach $14 trillion by end of 2023. USC Schaeffer. https://healthpolicy.usc.edu/article/covid-19s-total-cost-to-the-economy-in-us-will-reach-14-trillion-by-end-of-2023-new-research/
- World Health Organization. (2023). Who coronavirus (COVID-19) dashboard. World Health Organization. https://covid19.who.int/?mapFilter=deaths Muzumdar, J. M., &
- Muzumdar, J. M., & Cline, R. R. (2009). Vaccine Supply, demand, and policy: A Primer. Journal of the American Pharmacists Association, 49(4). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7185851/
- Lalani, H. S., Nagar, S., Sarpatwari, A., Barenie, R. E., Avorn, J., Rome, B. N., & Kesselheim, A. S. (2023, February 2). US public investment in development of mrna COVID-19 vaccines. the BMJ. https://www.bmj.com/content/bmj/380/bmj-2022-073747.full.pdf
- Wagner, C. E., Prentice, J. A., Saad-Roy, C. M., Yang, L., Grenfell, B. T., Levin, S. A., & Laxminarayan, R. (2020, December 1). Economic and behavioral influencers of vaccination and antimicrobial use. Frontiers. https://www.frontiersin.org/articles/10.3389/fpubh.2020.614113/full
- Gumbrecht, J., & Thomas, N. (2020, September 16). Federal government details plans to distribute free covid-19 vaccines. CNN. https://www.cnn.com/2020/09/16/health/coronavirus-vaccine-distribution-plan/index.html
- Schneider, E. C., Shah, A., & Sah, P. (2021, December 14). The U.S. covid-19 vaccination program at one year: How many deaths and hospitalizations were averted?. Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2021/dec/us-covid-19-vaccination-program-one-year-how-many-deaths-and
- Mathieu, E., Ritchie, H., Rodés-Guirao, L., Appel, C., Giattino, C., Hasell, J., Macdonald, B., Dattani, S., Beltekian, D., Ortiz-Ospina, E., & Roser, M. (2020, March 5). Coronavirus (COVID-19) vaccinations. Our World in Data. https://ourworldindata.org/covid-vaccination
- Bilinski, A., Emanuel, E., Thompson, K. (2023, January 3). Covid-19 and excess all-cause mortality in the US and 20 comparison countries, June 2021-March 2022. JAMA. https://jamanetwork.com/journals/jama/fullarticle/2798990
- Al-Zaman, S. (2021, January 1). Prevalence and source analysis of COVID-19 misinformation of 138 countries. IFLA Journal. https://journals.sagepub.com/doi/10.1177/03400352211041135
- Coleman, J. (2023, July 26). Global Vaccine Tracking. Morning Consult Pro. https://pro.morningconsult.com/trackers/global-vaccine-skepticism-tracker
- Freedman, R. (2023, August 23). Sweeping EU digital misinformation law takes effect. Legal Dive. https://www.legaldive.com/news/digital-services-act-dsa-eu-misinformation-law-propaganda-compliance-facebook-gdpr/691657/
- Brannon, V. C. (2022, August 1). False Speech and the First Amendment: Constitutional Limits on Regulating Misinformation. Congressional Research Service. https://crsreports.congress.gov/product/pdf/IF/IF12180
